A 46 year old male with complaints of spasms
July 13th,2023
This is an online e log book to discuss our patient de-identified health data shared after taking his/her/guardians signed informed consent. Here we discuss our individual patients problems with an aim to solve the patient’s clinical problem with collective current best evident based output.
This E blog also reflects my patient cantered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings,investigations and come up with diagnosis and treatment plan.
This is the case of 46 year old male farmer and JCB handler by occupation resident of chityala.
CHIEF COMPLAINTS :
Spasms in phalanges of all limbs and calf muscles since 10days.
Tremors of hands since 3days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 10years ago and went to hospital with complaints of stomach pain and vomitings and diagnosed with pancreatitis for which he undergone a surgery.
-8years ago he experienced weight loss and weakness, then he visited a hospital and there he was diagnosed with diabetes and started using oral hypoglycemics.
-His sugar levels were not controlled so he started using insulin.
-H/O seizures when RMP administered iv glucose and unknown inj into iv 4 months ago associated with up rolling of eye balls which lasted for 1min and 5episodes occurred in 30min. Between each episode he had no memory of seizure.
-H/O delusions at night for 3days when he stopped alcohol consumption.
-Complaints of spasms in all digits of limbs and calf muscles associated with severe pain which of squeezing type since 10days. Spasms occurred continuously for 10min for every episode and relieved on random movements of digits.
-Tremors in hands since 3days.
Past history:
-surgery for relieving nerve compression in front of neck due to heavy exercise 16years ago
-surgery for pancreatitis 10years ago
-k/c/o diabetes since 8years
-Achilles tendon repair in right leg due to trauma 8years ago
-ulcer formation on dorsal aspect of foot due to trauma 1year ago
-Visiting psychiatry for alcohol withdrawal sessions since jan 2023 for 4 months.
-N/K/C/O HTN,TB,asthma, epilepsy.
PERSONAL HISTORY:
Mixed diet
Adequate sleep
Normal appetite
Bladder and bowel moving are normal
No known allergies
H/O smoking since 10years,1 pack(10) a day
H/O alcohol consumption since 10years consuming quarter/half a day continuously for a week and discontinued for 1 or 2 months. He had withdrawal symptoms in between.He missed his insulin shots when he consumed alcohol.
FAMILY HISTORY:
No significant family history.
Daily routine:
-Before DM-6 years back he used to do JCB business.He wakes up at 7 .Goes from nkp to kattangur, before having bf.He usually has his bf at 10 and lunch at 2pm .He comes back at 8-9pm ,has his dinner at and sleeps around 10 am. One day all of the sudden loss of weight for which he went to a local hospital (yashoda) and was found to have DM type 2 (540mg/dl) and was given medication( insulin).He stopped going to work since then and took rest at his home.
-After DM-Patient wakes up at 4 am in the morning and collects milk from buffalos and come back to home by 7.30 and supply milk till 9.30am.Takes his breakfast at 10 am and
then takes rest.He has lunch at 1 pm and takes afternoon nap.At 4pm again he goes to buffalo farm and collects milk and supply.Comes back to home by 7.30 he will have his dinner by 9pm and goes to bed by 10pm.
GENERAL EXAMINATION:
Patient is examined in the well lit room with the consent.
Patient is conscious, coherent and cooperative.
No pallor, icterus, clubbing, cyanosis, bipedal edema and generalised lymphadenopathy.




VITALS:
Temp- Afebrile
BP-120/80 mmhg
PR-80bpm
RR- 16cpm
Spo2- 98% at room air
GRBS:282mg/dl
SYSTEMIC EXAMINATION:
CVS:
Inspection -
Chest wall is bilaterally symmetrical
No precordial bulge is seen
Palpation-
JVP- Normal
Apex beat-palpated
Auscultation-
S1&S2 are heard
No murmurs
RESPIRATORY SYSTEM:
Position of trachea- central
Bilateral air entry, normal vesicular breath sounds are heard.
No added sounds
CNS:
Higher mental functions are present.
Patient is conscious ,coherent and co operative, well oriented to time and space.
Speech normal.
Motor and sensory system- Normal
Reflexes- Right Left
Biceps +2 +2
Triceps +2 +2
Knee +2 +2
Ankle 0 0
Cranial nerves - intact
PER ABDOMEN:
Inspection:
Visible scar of 10cm due to pancreatitis surgery
All quadrants are moving equally with respiration
Umbilicus - central and inverted
No engorged veins, prominent Venous pulsations and visible peristalsis.
On palpation:
Superficial palpation- No Local rise in temperature and no tenderness.
Deep palpation- No guarding, rigidity.
On percussion:
Tympanic note - heard on all quadrants
On auscultation:
Bowel sounds heard
Investigations:
Complete urine examination-

Glycated hemoglobin-

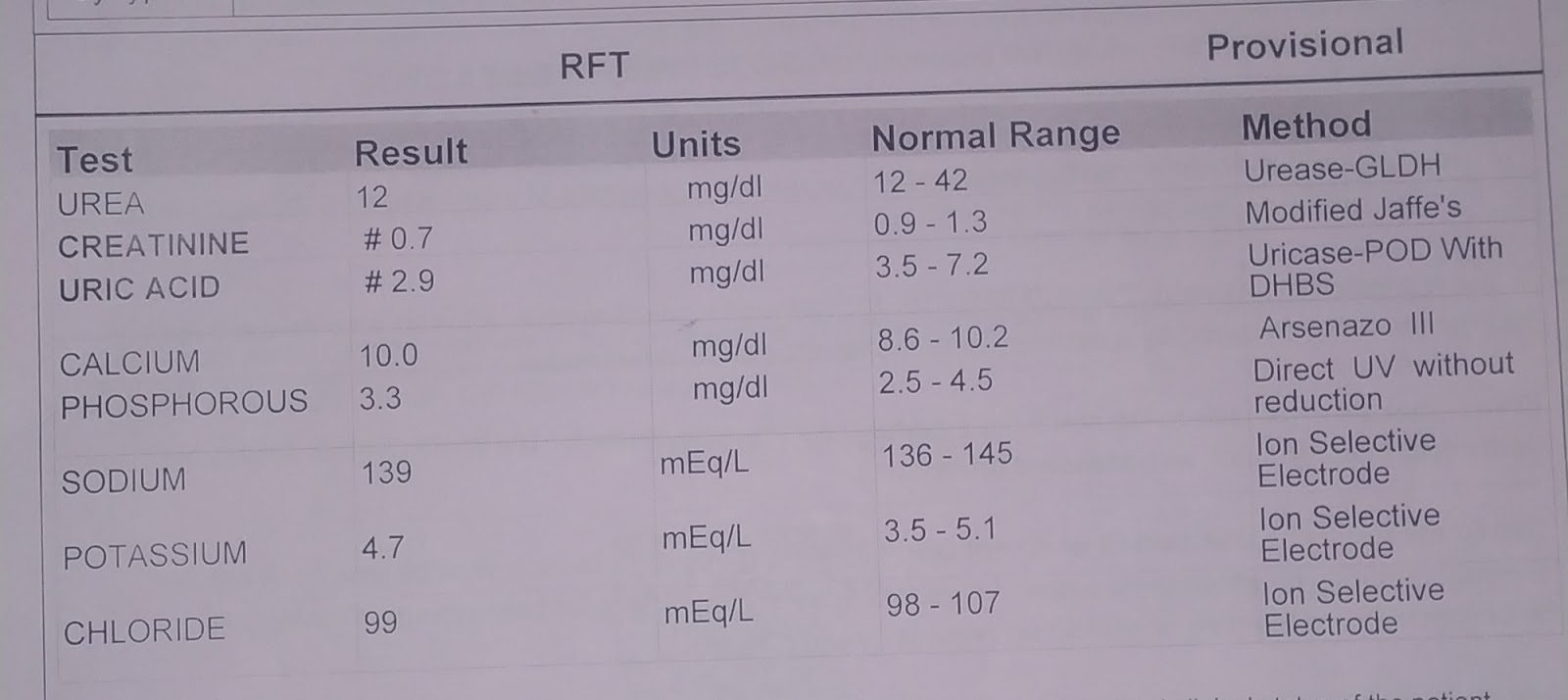
Renal function tests-
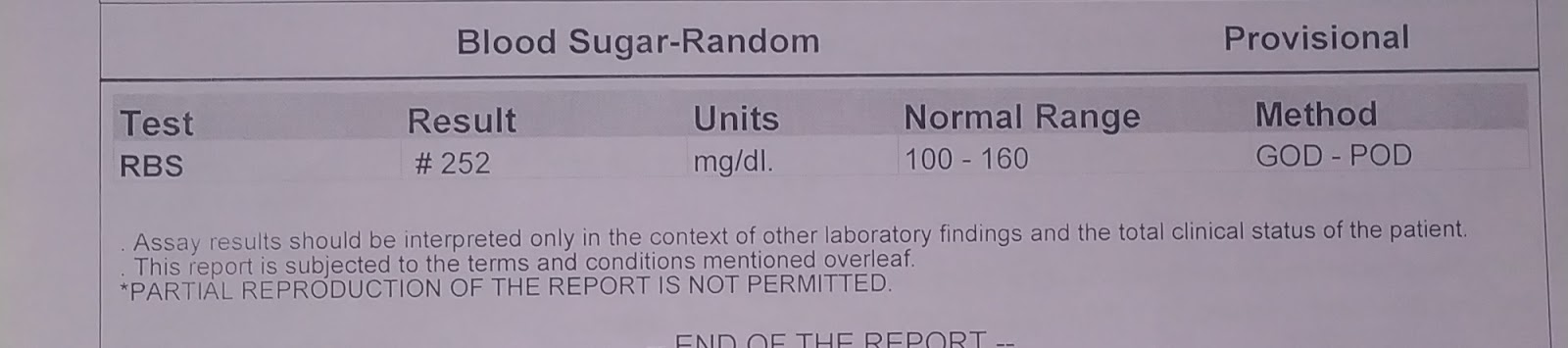
GRBS-
2D echo-

Provisional diagnosis:
Spasms due to alcohol withdrawal.



Comments
Post a Comment