A 60year old chronic alcoholic male presented to the OPD with distended abdomen
8th july, 2023
This is an online e log book to discuss our patient de-identified health data shared after taking his/her/guardians signed informed consent. Here we discuss our individual patients problems with an aim to solve the patient’s clinical problem with collective current best evident based input.
This E blog also reflects my patient cantered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings,investigations and come up with diagnosis and treatment plan.
This is the case of 60year old male farmer and carpenter by occupation and resident of Guramguda.
CHIEF COMPLAINTS :
-Abdominal distension since 4months
-Swelling of bilateral lower limbs since 4 months
-decreased urine output since 4months.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 4months back. He then developed abdominal distension which is insidious in onset and associated with pain which is stabbing type ,aggravated on eating and no relieving factors.
-H/O swelling in both legs upto level of knees associated with dragging type of pain since 4months.
-H/O decreased urine output since 4months.
-H/O SOB since 4months
-Patient then went to a hospital and on medication complaints were subsided. He developed the same complaints 10days back and came to the our OPD hospital yesterday(i.e 7th july 2023).
-H/O chronic cough since 4months with whitish sputum.
-H/O burning micturition since 1month.
-H/O intermittent fever since 10 days associated with chills and rigors relieved on medication.
-Other complaints- presence of spherical swelling insidious in onset (1month ago) infront of leg 9inches from the lower border of patella initially in the size of a peanut and progressive to the current size measuring 3x3cm. The swelling is tender, firm in consistency and no mobility and punctum is seen.
No H/O nausea, vomitings , chest pain , palpitations, giddiness , sweating and jaundice.
Past history:
H/O 2episodes of seizures 12years ago controlled by medication.
H/O spasms of both limbs phalanges
K/C/O Type 2 DM and HTN since 6years.
N/K/C/O- TB, asthma, CVA , CAD , Thyroid disorders.
Surgical history-cataract removal for one eye 2years ago and other eye 1year ago.
-Removal of cyst like swelling present between two eyebrows 1year ago.
Treatment history-H/O blood transfusion done 3months back-uneventful
PERSONAL HISTORY:
Mixed diet
Decreased appetite since 2months
H/O constipation since 1 month, passing stools once in 3days and decreased urine output since 4months with burning micturition since 1month.
Adequate sleep
Addictions-Chronic alcoholic since 40years(around 180ml/day) and chronic smoker since 40years(one pack of beedi per day containing 18 beedis)
FAMILY HISTORY:
No significant history
GENERAL EXAMINATION:
Patient is examined in the well lit room with the consent.
Patient is conscious, coherent and cooperative.
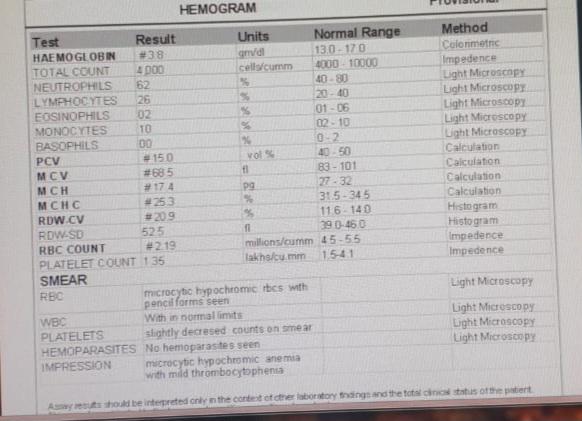
Pallor present

Bipedal edema -present pitting type


No signs of icterus, clubbing, cyanosis, lymphadenopathy.



VITALS:
Temp- Afebrile
BP-140/70
PR-105bpm
RR-24cpm
Spo2-96% at room air
GRBS:485mg/dl
SYSTEMIC EXAMINATION:
CVS:
Inspection -
Chest wall is bilaterally symmetrical
Ne precordial bulge is seen
Palpation-
JVP- Normal
Apex beat-palpated in 5th intercostal space in mid clavicular line
Auscultation-
S1&S2 are heard
No murmurs
RESPIRATORY SYSTEM:
























Comments
Post a Comment