A 57 year old man came to OPD with complaint of one episode of seizures.
July 27th,2023
This is an online e log book to discuss our patient de-identified health data shared after taking his/her/guardians signed informed consent. Here we discuss our individual patients problems with an aim to solve the patient’s clinical problem with collective current best evident based output.
This E blog also reflects my patient cantered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings,investigations and come up with diagnosis and treatment plan.
This is a case of 57 years old man auto driver by occupation.
CHIEF COMPLAINTS:
-1 episode of seizure yesterday morning at 7:30AM.
HISTORY OF PRESENTING ILLNESS:
-Patient was apparently normal until yesterday morning then he developed stiffness of all four limbs and neck for 10minutes associated with up rolling of eyes, frothing from mouth and involuntary micturition.
-No involuntary defecation present.
-No memory of the incident occurred.
-No history of fever, headache, vomitings.
PAST HISTORY:
-Patient had a friendly fight at age of 15years and fell down on road hitting his head associated with swelling and no external bleeding present.
-4years ago with little experience of loss of memory and blurring of vision he went to doctor and CT was done. Doctor told him there was a clot in his head and prescribed medicines which patient used for 5months.
-3years ago patient had right eye cataract surgery.
-N/K/C/O DM, TB, epilepsy, CVA, CAD, thyroid disorders and bronchial asthma.
FAMILY HISTORY:
No significant family history.
PERSONAL HISTORY:
Diet :Mixed
Apetite:Normal
Bowel and bladder Movements:Regular
Sleep:Adequate
Addictions occasional alcoholic, regular beedi smoker 10-15/day since 12years.
No allergies
Daily routine: Patient wakes up at 4am and does a few household chores along with his wife untill 7am and relaxes between 7am to 9 am. He goes to his work by 10am and has his lunch at 2 pm, continues work upto 5:30 and returns home at 6pm and has tea and watches television until 7pm. Has dinner by 9:30, sleeps by 10 pm.
All of a sudden prior to his admission in the hospital, patient experienced stiffness of all four limbs and frothing through his mouth for approximately 15mins at 7:30 Am in the morning, for which he was taken to a government hospital nearby and was given treatment and was reffered to our hospital.
No change in daily routine due to his seizures.
GENERAL EXAMINATION:
Patient was examined in well lit room with consent.
On examination patient is conscious, coherent, cooperative.
No pallor, icterus, cyanosis, clubbing, lymphadenopathy and edema present.






VITALS:
Temperature-Afebrile
PR-82bpm
RR: 14Cpm
BP:130/80mm Hg
Spo2:99% at room air
GRBS charting: 98mg/dL
SYSTEMIC EXAMINATION:
CVS:
S1S2 heard.
No murmurs present.
RS:
Bilateral symmetrical chest expansion present.
Bilateral air entry is present.
Normal vesicular breath sounds are heard.
Per abdomen:
Soft and Nontender.
All quadrants equally moving with respiration.
No abdominal distension.
CNS:
Higher mental functions present.
Cranial nerves intact and normal.
Motor system:
Right Left
Tone-
UL rigid rigid
LL rigid rigid
Reflexes- Right Left
Biceps +2 +2
Triceps +2 +2
Knee 0 0
Ankle 0 0
Sensory system is normal.
Mini mental score:
28/30.
PROVISIONAL DIAGNOSIS:
Seizures under evaluation.
INVESTIGATIONS:
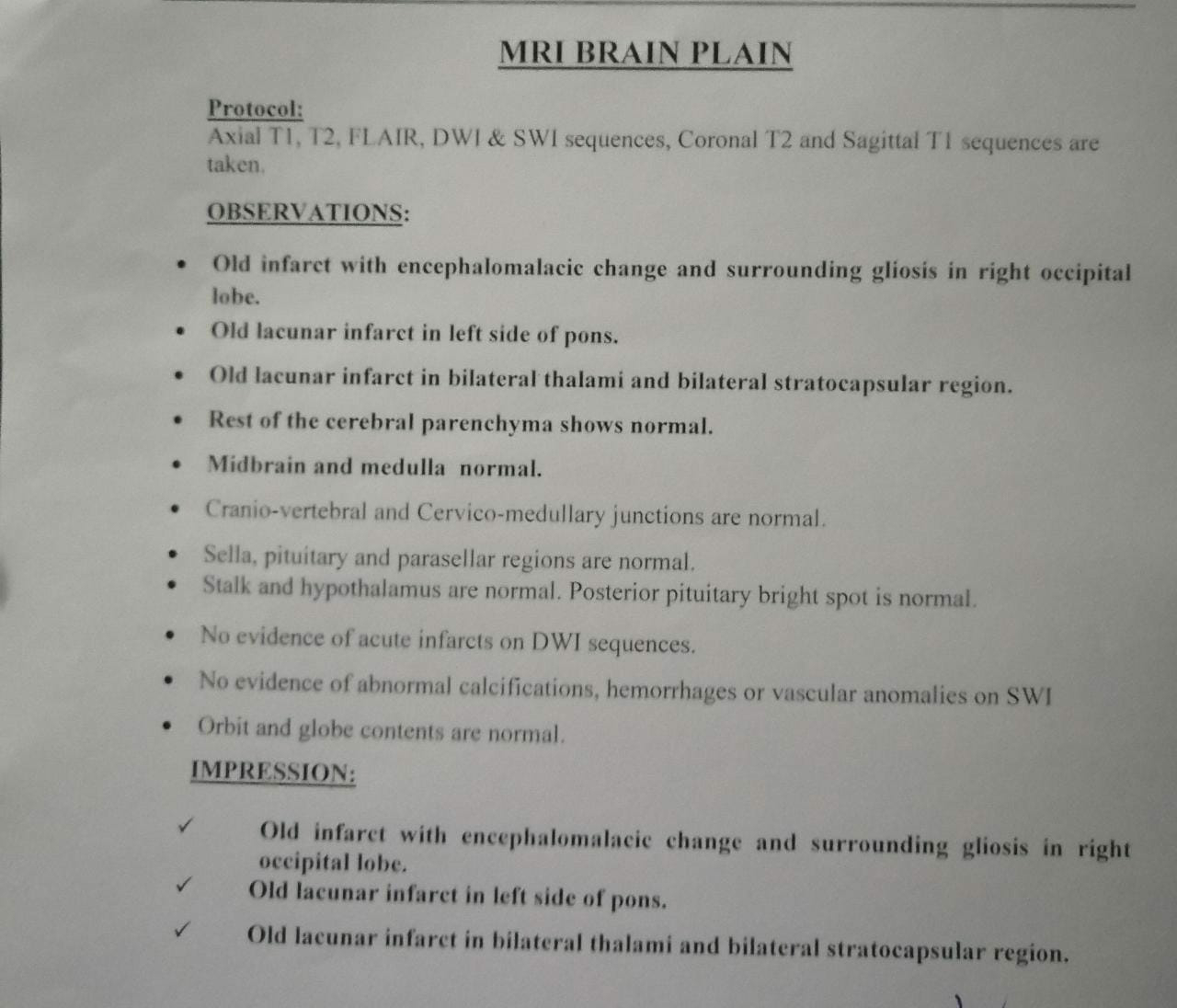
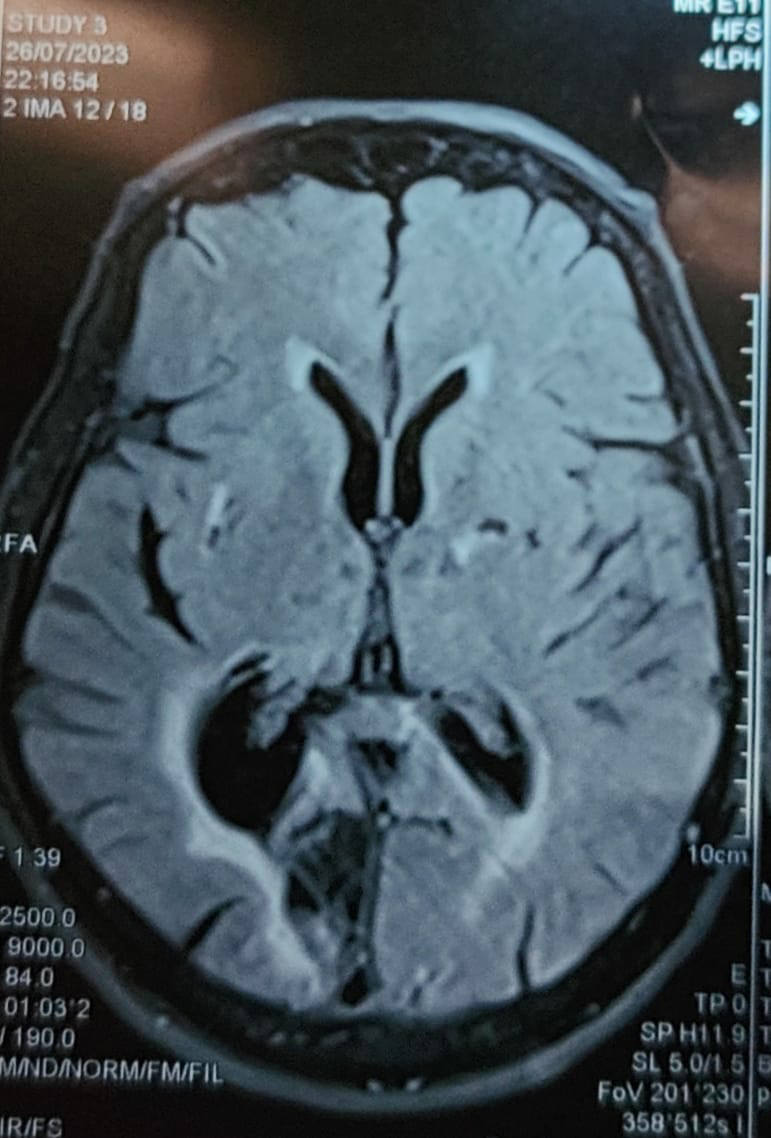
MRI brain:
Hemogram:

CUE:

LFT:

Sr.creatinine:

BGT:

Urea:

Serum electrolytes:

RBS:

ECG:

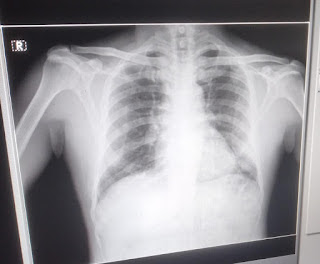
Chest Xray:
2D echo:

Serology:



Treatment:


Comments
Post a Comment